






This transcript has been edited for clarity.
Rebecca F. Neustein, MD: Good evening. I’m Rebecca Neustein, MD, from Emory Eye Center, here at the American Glaucoma Society meeting, and Dr. Arcalas, one of our PGY-2 residents, is going to be presenting our project on surgical success following cataract surgery in combination with the Omni surgical system (Sight Sciences) compared with Kahook dual blade (KDB; New World Medical) goniotomy.
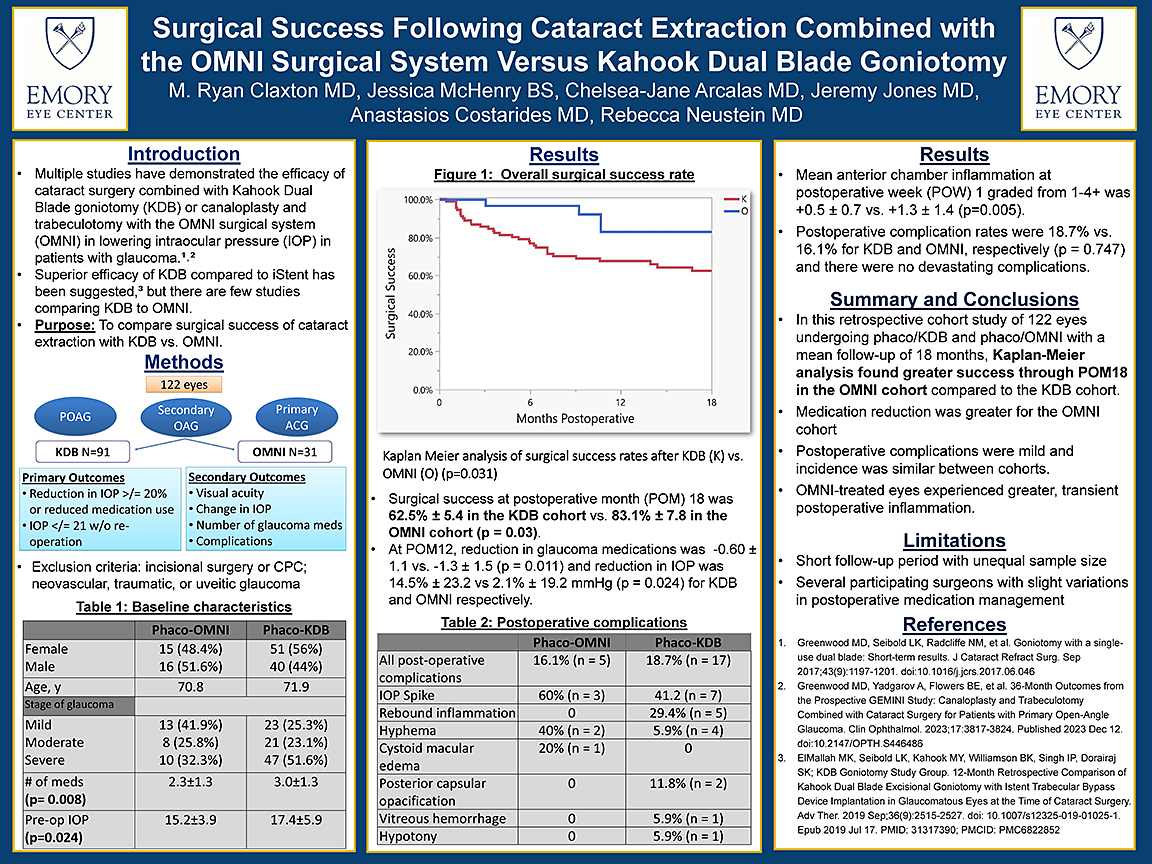
Chelsea-Jane Arcalas, MD: Thank you, Dr. Neustein. Again, I’m Dr. CJ Arcalas, one of the PGY-2s at Emory. I have the pleasure of presenting our data and our research here. We wanted to look at surgical success, and as Dr. Neustein said, our goal was to compare surgical success of cataract extraction with Omni and KDB. In this retrospective cohort study of 122 eyes, we looked at patients with primary open-angle glaucoma, secondary open-angle glaucoma, and primary angle-closure glaucoma. We looked at 122 eyes. There were 91 patients undergoing phaco+KDB, as well as 31 eyes undergoing phaco+Omni. The primary outcome was to look at surgical success, which under the definition of the AGS preferred practice panel, is defined as reduction in IOP ≥20%, or reduced medication use as well as IOP ≤21 mmHg without reoperation.
And of course, other secondary outcomes like visual acuity, changing IOP, number of glaucoma meds, and other complications as well. Exclusion criteria includes [prior] incisional surgery or cyclophotocoagulation, neovascular glaucoma, traumatic glaucoma, things like that. And then we have our baseline characteristics here.
Really the biggest things that we found was that, after doing a Kaplan-Meier analysis of surgical success, there was a statistically significant difference between KDB and Omni (P=.03), where surgical success at postoperative month 18 was 83.1% in the Omni cohort and 62.5% in the KDB cohort. Also, we found that there was a statistically significant reduction in glaucoma medications. There was more of a reduction in the Omni group, with a reduction of 1.3 medications in that group, as well as a reduction in medications of 0.6 in the KDB group, which was statistically significant. There was also a reduction in IOP in general.
In general, the confidence interval is quite wide in this, which may suggest a similar on average reduction in IOP, but still statistically significant as well. We have a table of our different postoperative complications here. The rate is similar, 16% in the phaco+Omni group; in the phaco+KDB group it was about 18%. No devastating complications, but like I said, very similar rates amongst the groups.
What we found and what we wanted to focus on was the fact that the greater surgical success rate was found in the Omni group through postoperative month 18 with similar IOP reduction and greater medication reduction in the Omni cohort.
We wanted to touch on the limitations as well regarding short follow-up period with unequal sample size. We’d love to get more numbers in the Omni group. Also, there were several participating surgeons who of course manage things differently in the postoperative setting in terms of their medications and drops.
Thank you for having us and thank you for listening to our research.
Dr. Neustein: I’d like to credit Ryan Claxton, MD, one of our PGY-4 residents who also led this project, as well as Jessica McHenry and my partners, Jeremy Jones, MD, and Anastasios Costarides, MD, who also participated. Thank you. GP