


For Glaucoma Physician’s Surgical Pearls video series, Kateki Vinod, MD, demonstrates the use of a scleral plug to close the limbal fistula during removal of an exposed glaucoma drainage implant. Transcript of the narration follows below:
This is Kateki Vinod, a glaucoma specialist at the New York Eye and Ear Infirmary of Mount Sinai.
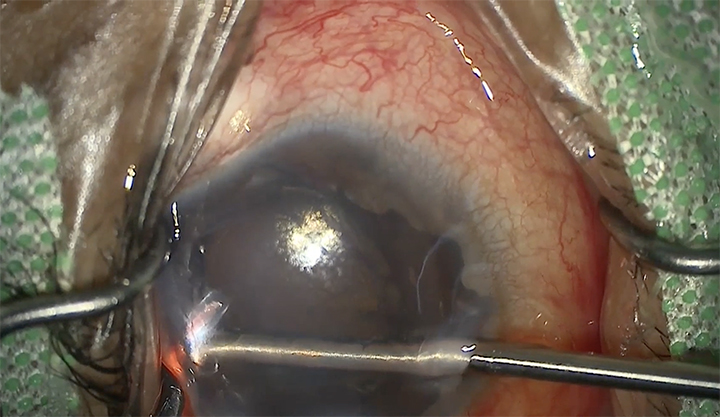
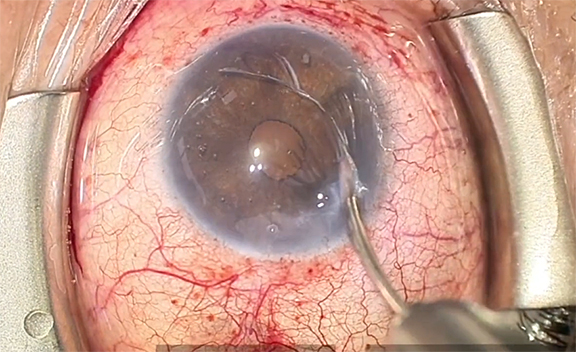
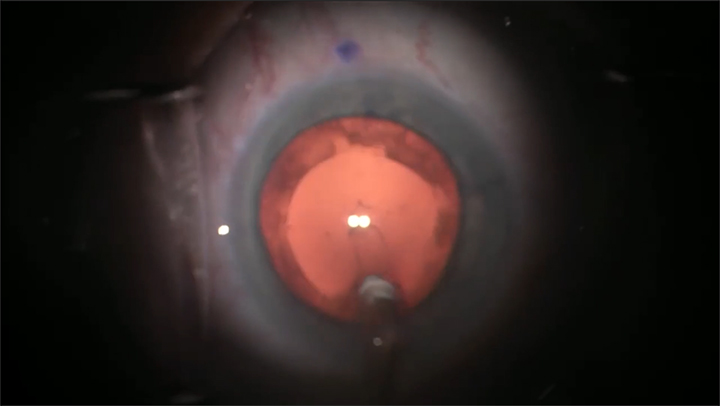
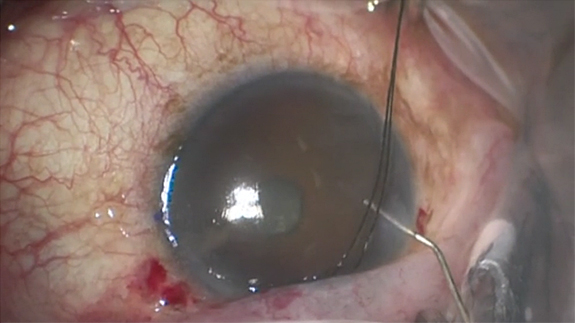
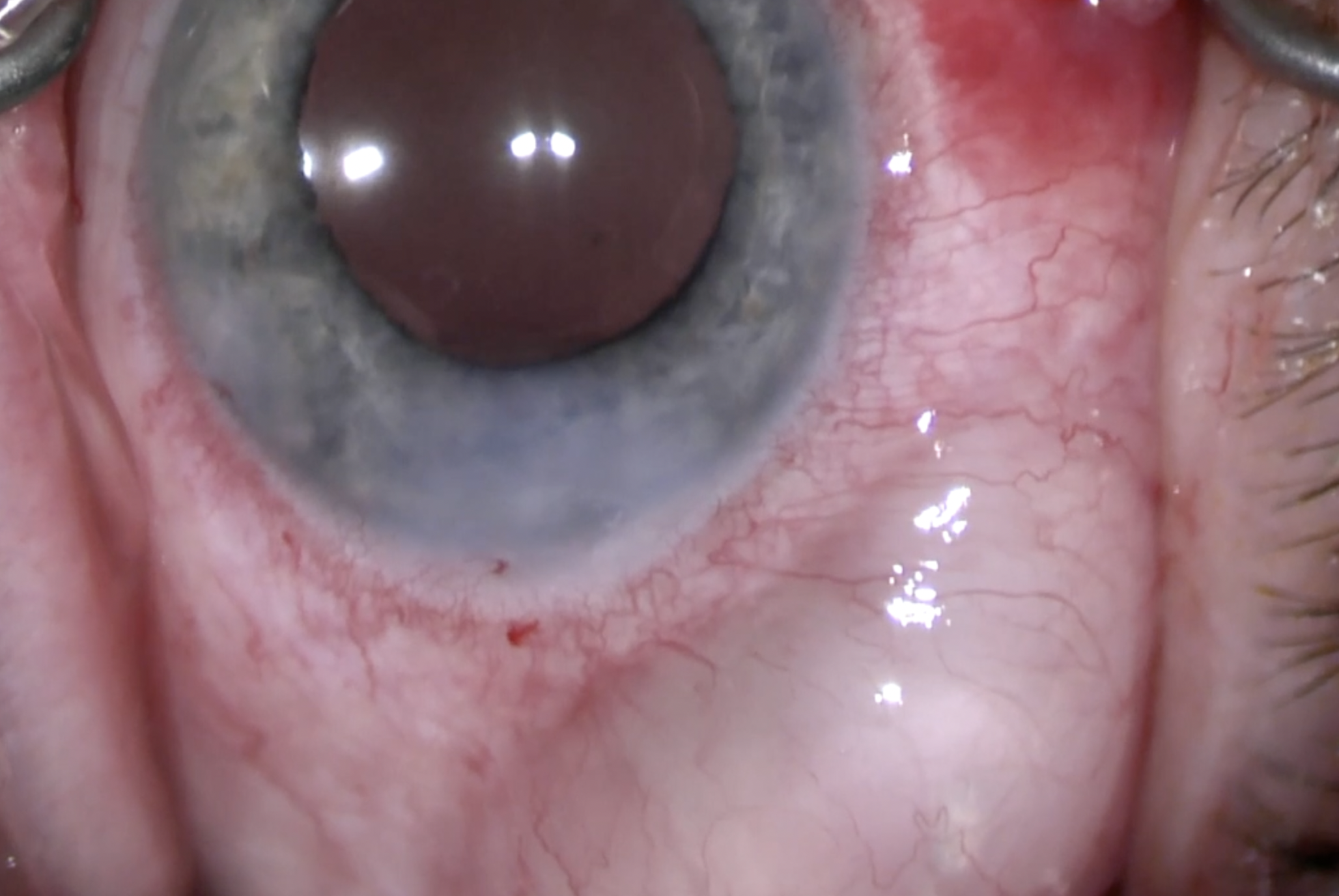
This is a monocular patient who had undergone placement of an inferotemporal and inferonasal tube shunt in his only seeing eye by his referring doctor. He developed a sizable conjunctival erosion overlying the tube-plate junction of the inferonasal implant, which had migrated anteriorly toward the limbus. The referring surgeon attempted to revise this several times, but the inferonasal tube ultimately had to be removed. This video features a surgical technique developed by Dr. Paul Sidoti to close the scleral fistula during tube shunt removal or repositioning.1
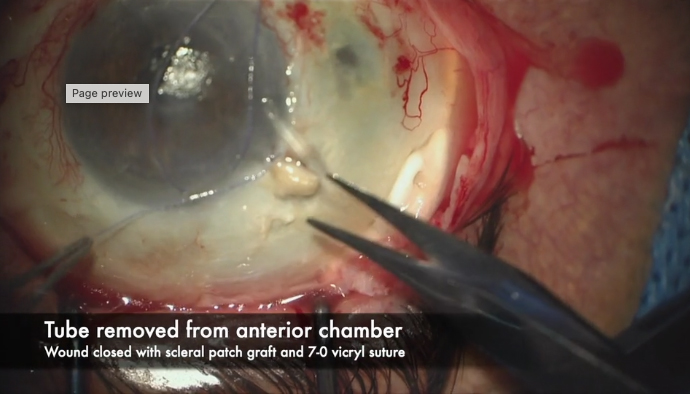
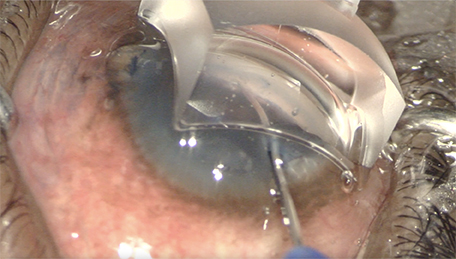
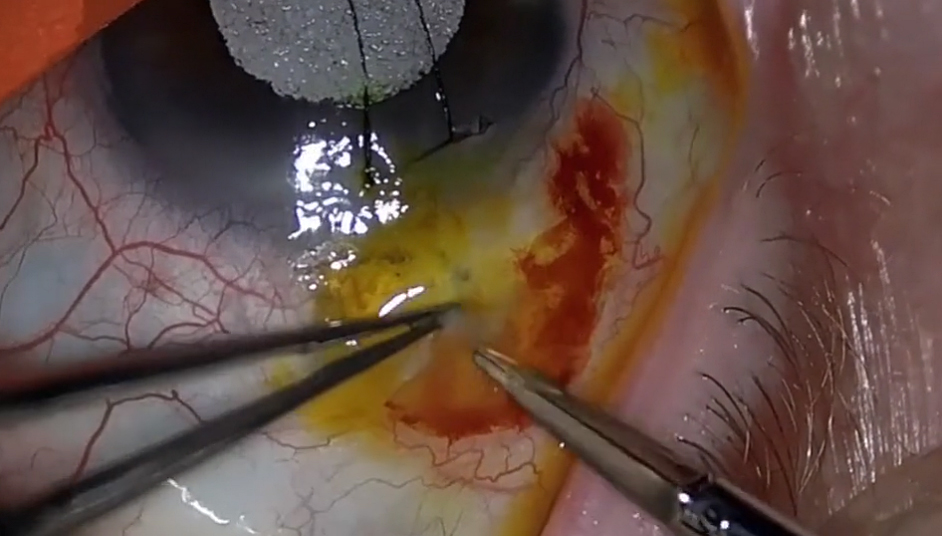
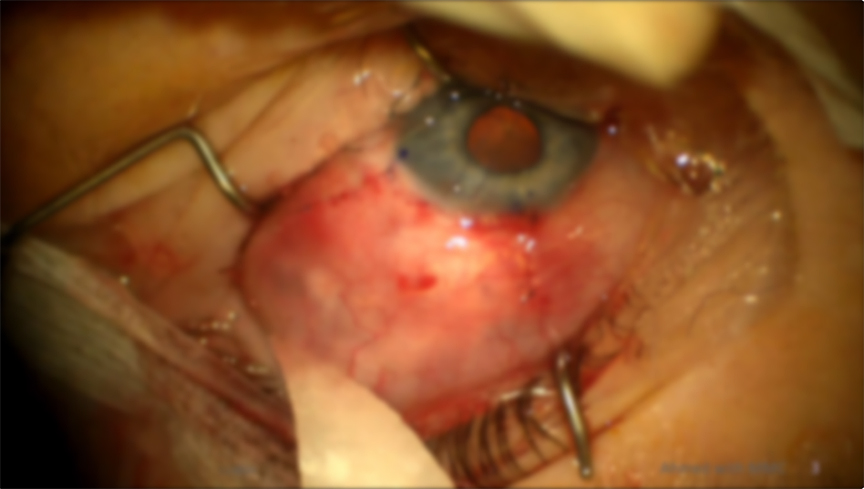
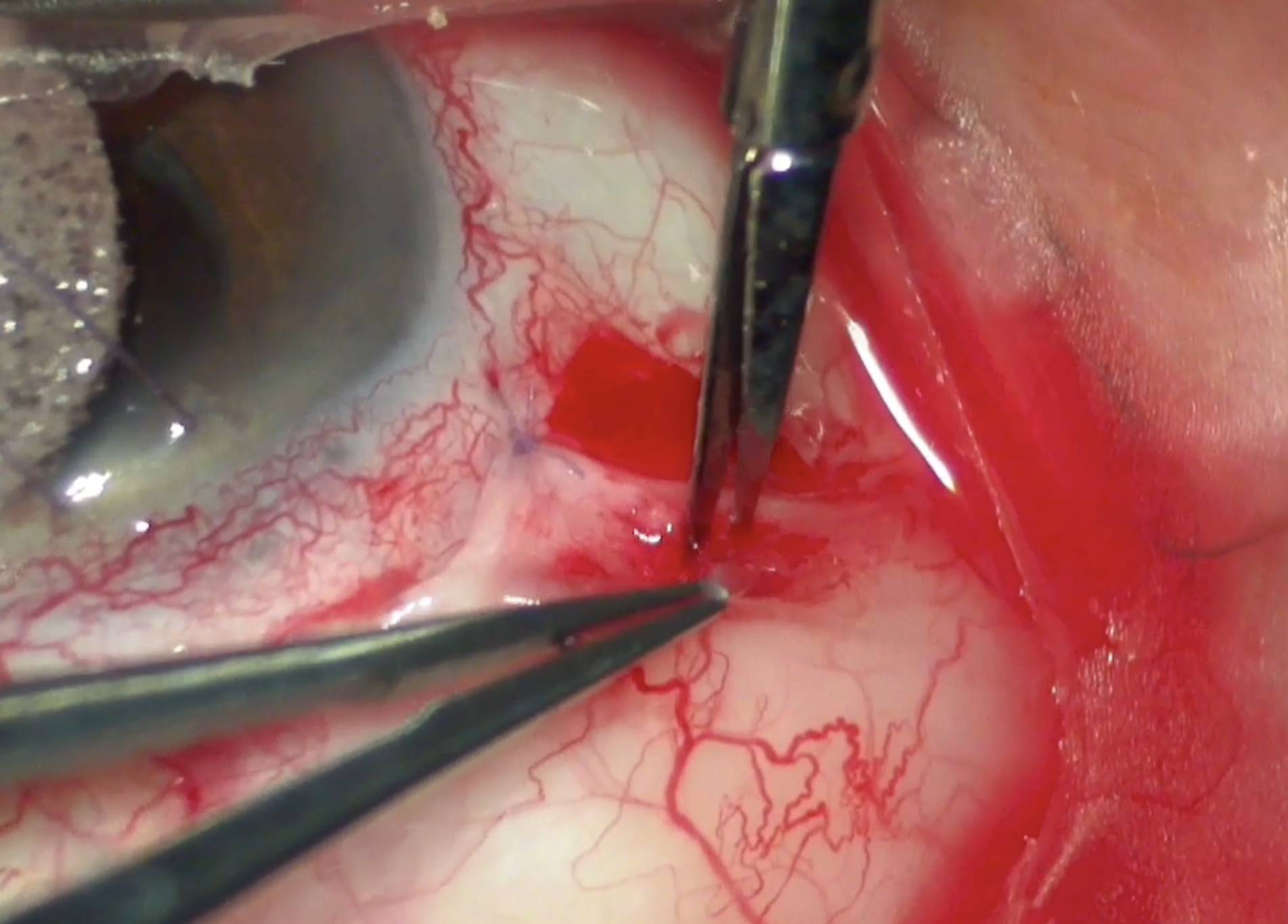
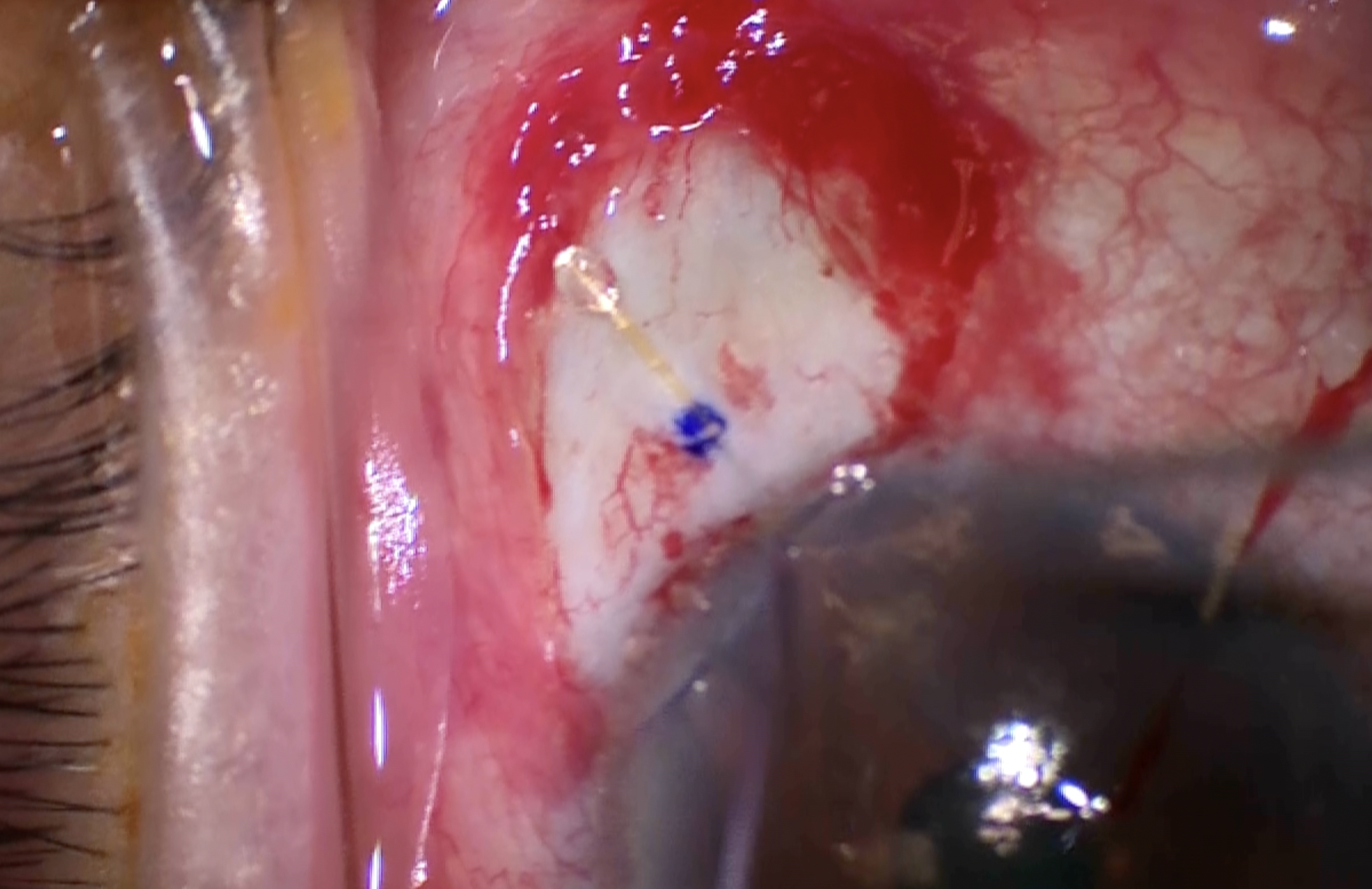
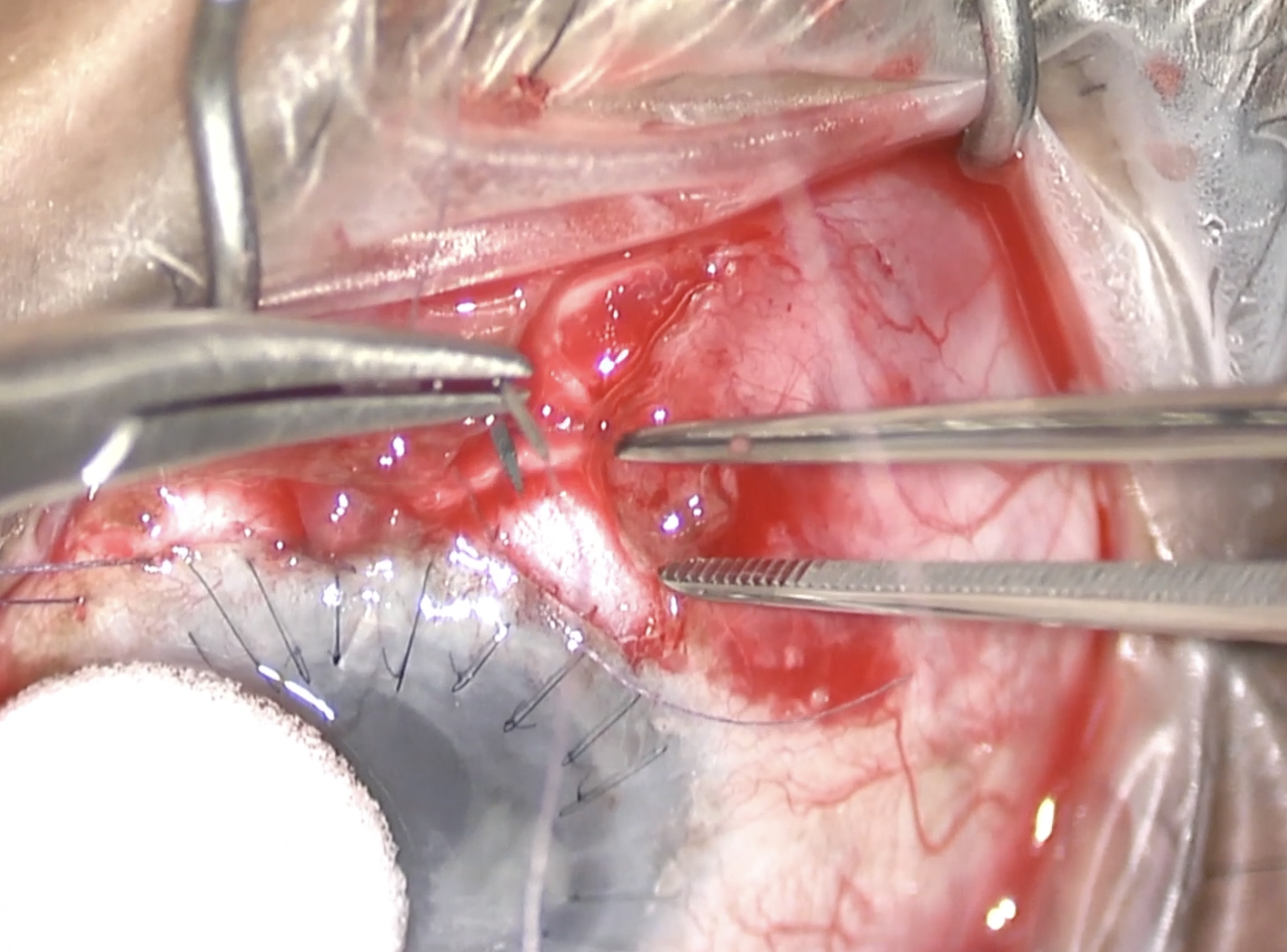
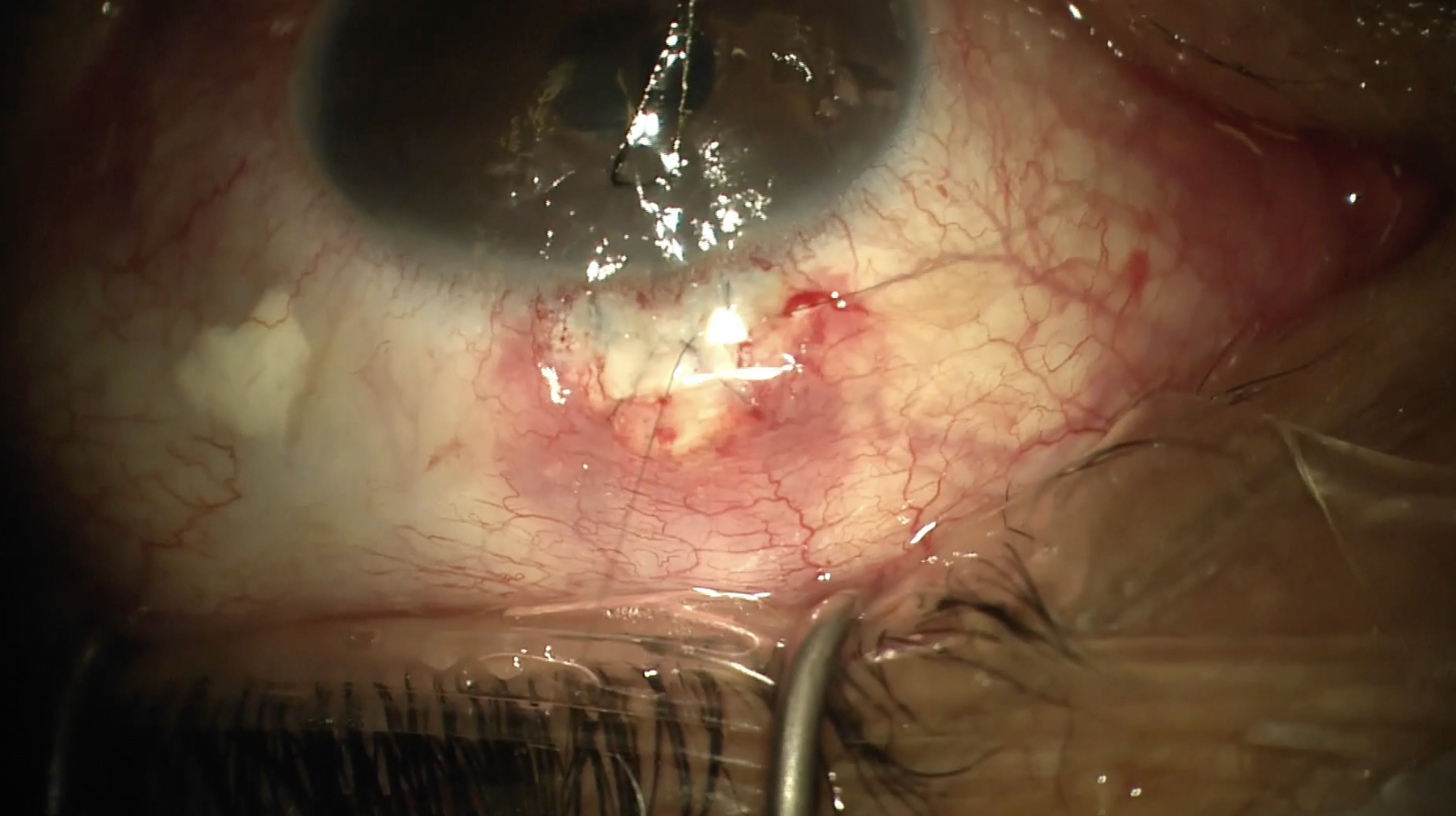
Extensive conjunctival scarring is present as would be expected after multiple previous attempts at revision. The case begins in standard fashion with the creation of a limited peritomy using the existing conjunctival erosion as a starting point. Generous cautery is performed to remove any epithelial cells and achieve hemostasis. After incision and removal of the fibrous capsule surrounding the tube, a figure-of-eight 8-0 Vicryl suture is pre-placed adjacent to the extraocular portion of tube at the limbus in preparation for closure of the scleral fistula. Pictured here is Tutoplast sclera, a dehydrated human tissue allograft, which has been fashioned into a triangular wedge which will be used to plug the scleral fistula. The scleral plug is kept dry until it's ready for use and in this case the tip of the plug is trimmed to an appropriate length for insertion into the anterior chamber. In one swift motion, the tube is removed from the anterior chamber, and the scleral plug is inserted into the fistula where it immediately hydrates, expands, and occludes the opening. The suture is then tied off in 3:1:1 fashion, achieving watertight closure. An additional suture or fibrin glue may be used to further reinforce the closure. This technique is preferred over direct suture closure of the fistula as the latter may induce irregular astigmatism or leave a wound leak. The remainder of the case proceeds by cutting each of the stalks of connective tissue that have grown through the 2 anterior eyelets as well as the 4 fenestrations on the endplate until the endplate is completely freed and removed from the surgical field. Finally, the case concludes with reapposition and closure of the conjunctival flaps with 8-0 Vicryl suture.
Thanks very much for your attention and a special thank you to Dr. Sidoti. GP
References
1. Panarelli JF, Banitt MR, Sidoti PA. Scleral fistula closure at the time of glaucoma drainage device tube repositioning: a novel technique. Arch Ophthalmol. 2012 Nov;130(11):1447-51.

Other Videos From Series